Project Highlights



What is Laryngoscopy?
Laryngoscopy is the endoscopy of the larynx, a part of the throat. It is a medical procedure that is used to obtain a view, for example, of the vocal folds and the glottis. The larynx is located at the top of the trachea and is your voice box. Laryngoscopy may also be performed to facilitate tracheal intubation during general anaesthesia or cardiopulmonary resuscitation.


Functions & Context of Laryngoscopy

Diagnostic
This device can be used to look for the causes of symptoms in the throat or voice box (such as trouble swallowing or breathing, voice changes, bad breath, or a cough or throat pain that won't go away. It can also be used to take a better look at abnormal masses in the vocal cords or nearby parts of the throat and take biopsy samples for examination.

Operative
Long thin instruments can be passed down the laryngoscope to remove small growths (tumors or polyps) on the vocal cords. A small laser on the end of the laryngoscope can also be used to burn away any abnormal areas. Operatively laryngoscopes are mainly used by otorhinolaryngologists to perform endolaryngeal microsurgery, such as removal of benign vocal fold lesions.

Intubation
Intubating laryngoscopes are used mainly by resident anaesthetists or nurses to expose a patient's trachea opening for ease of tracheal intubation to maintain efficient ventilation. It is one of essential tools for enabling anaesthetists to secure the airway and care for anaesthetised or critically ill patients. Intubating laryngoscopes are also called anaesthetic laryngoscopes by anaesthetists.
Market Research
Product Benchmarking
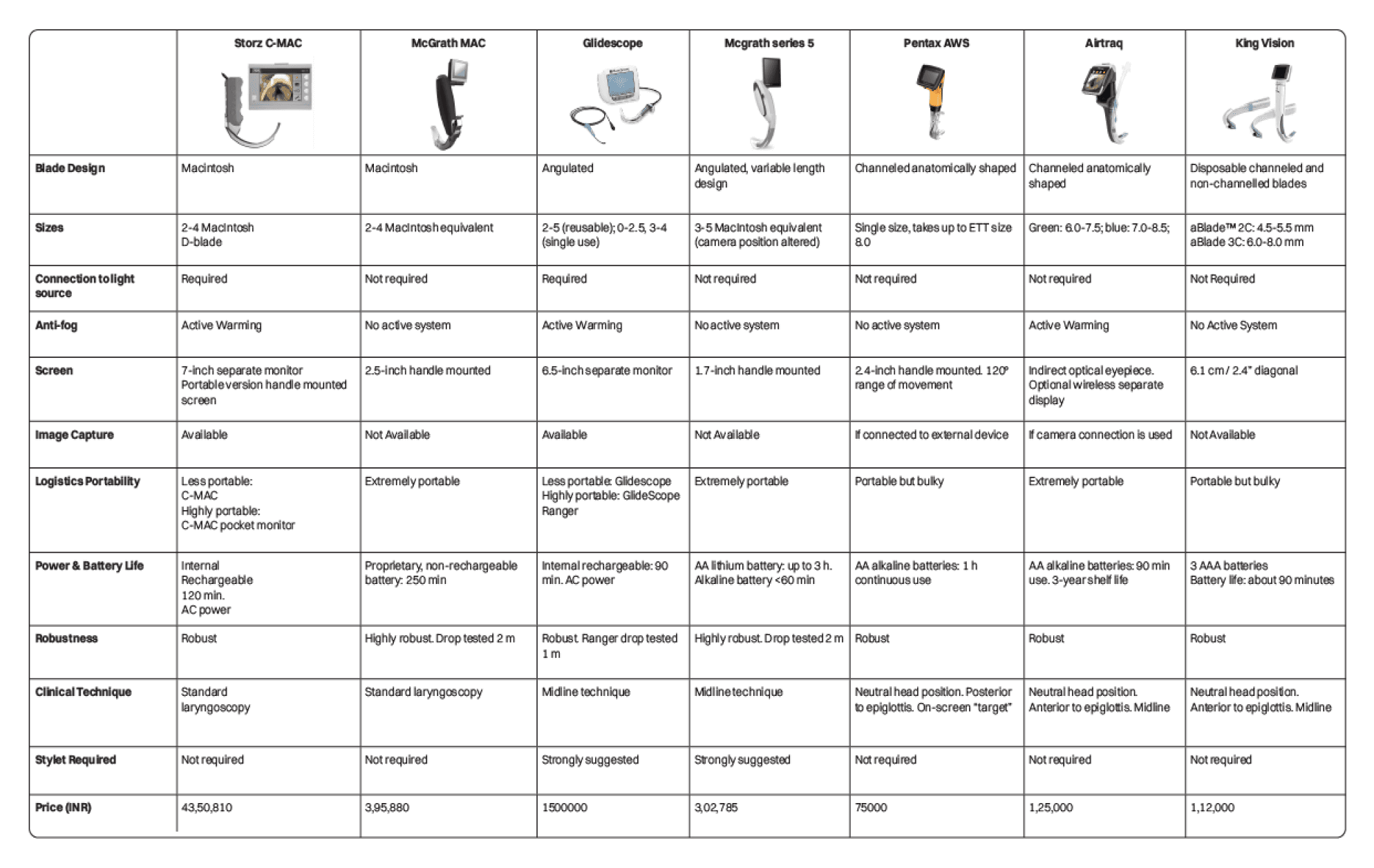
Before beginning to devise a new approach and concepts, it was crucial to understand the characteristics of existing market offerings and pinpoint their pros and cons. As a result, I performed exhaustive market research and benchmarked several products and compared them across various parameters.
Hospital Segmentation
Moving beyond the traditional segments based on demography (number of beds) including behaviours around quality, provides a more accurate and predictive segmentation. The following segments are - Leaders, Progressives and Community Hospitals.

Leaders
These hospitals have taken the lead in improving quality to global standards and in enhancing patient and healthcare worker safety — and they have targeted the uppermost socio-economic strata of Indian society, as well as medical “tourists,”. These corporate chains, often listed on India’s stock exchange, have one or two large tertiary care hospitals in top cities and a network of smaller primary and secondary care facilities that feed patients into the mother facility. Most patients at these facilities are paying out-of-pocket or via private insurance.

Progressives
These hospitals are often underestimated or ignored by western companies and are called the Progressives. These hospitals, of similar size (100 to 500 beds) as the Leaders, serve the upper and middle class. As the deep-pocketed Leader hospitals expand their services into the market that used to be dominated by the progressives, the progressives often respond by taking loans or private equity funding to upgrade their quality of care and their equipment. Therefore, they can be good candidates for innovative medical device vendors

Community Hospitals
The third and final segment of private hospitals comprises 70 percent of the hospital beds in India, but has less than a hundred beds per location. We estimate that there are over 40,000 such Community Hospitals, or “nursing homes,” as they are called in India. With an average of about 25 beds each, these facilities are typically run by a physician-turned-entrepreneur, who might also be the buyer and the key decision-maker for any Western-origin products and services. Most patients of these nursing homes are middle class or working class families who pay out of pocket.
User Research Methodology
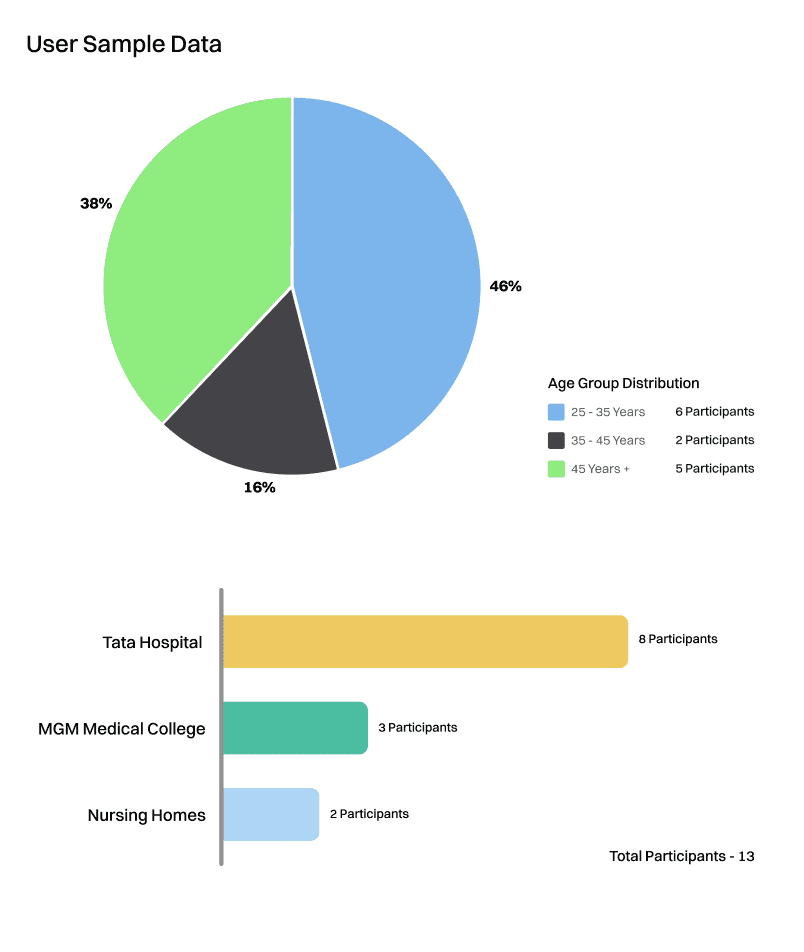
For my user research, I conducted a qualitative round of interviews with a sample size of 13 people. I was able to talk to a wide variety of people from senior professors to doctors currently pursuing their MD. As depicted in the age group distribution graph I had a good mix of young and upcoming doctors as well as senior experienced doctors who have been in the field for a long time. Most of these doctors were from Tata Memorial Hospital and MGM Medical College and two doctors working for nursing homes based in Bangalore. My primary focus was on anaesthetists since they are the primary users of this product.

For all the 13 user interviews, the data was recorded as shown in the image above. All the interviews were conducted digitally over a video call and recorded for future reference. After each interview, an immediate debrief was done as represented in the post-its above and then a deeper synthesis of their answers for each of the questions was recorded with reference to the recorded video. Along with a questionnaire I also conducted a card sorting exercise where I showed them pictures of the four most popular laryngoscopes and asked them to rate them to get a deeper understanding of their preferences regarding features, form and overall usage of video laryngoscopes. This helped me narrow down what the user's needs and pain points are to further consider for my design intervention.
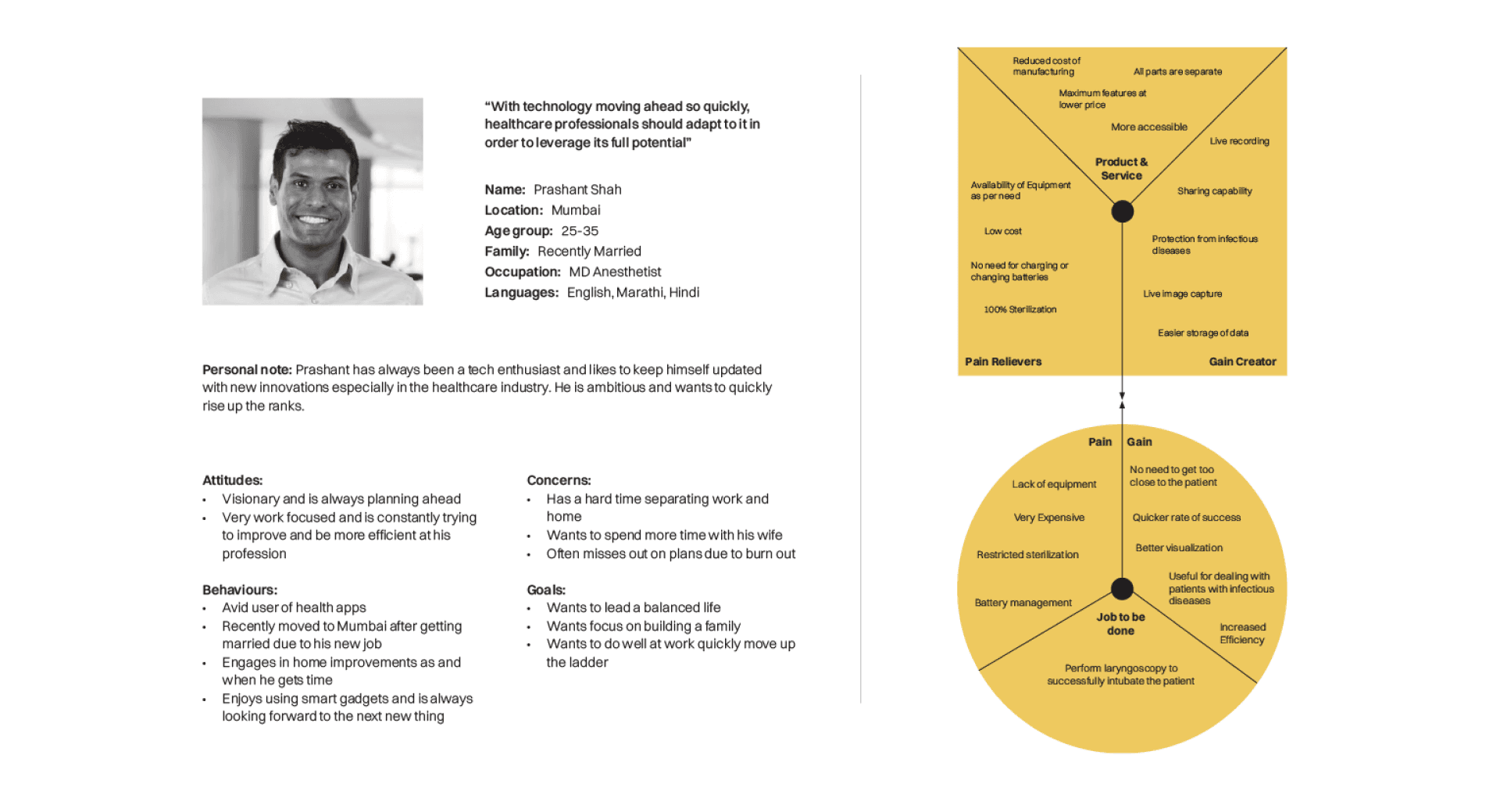
User Persona 1
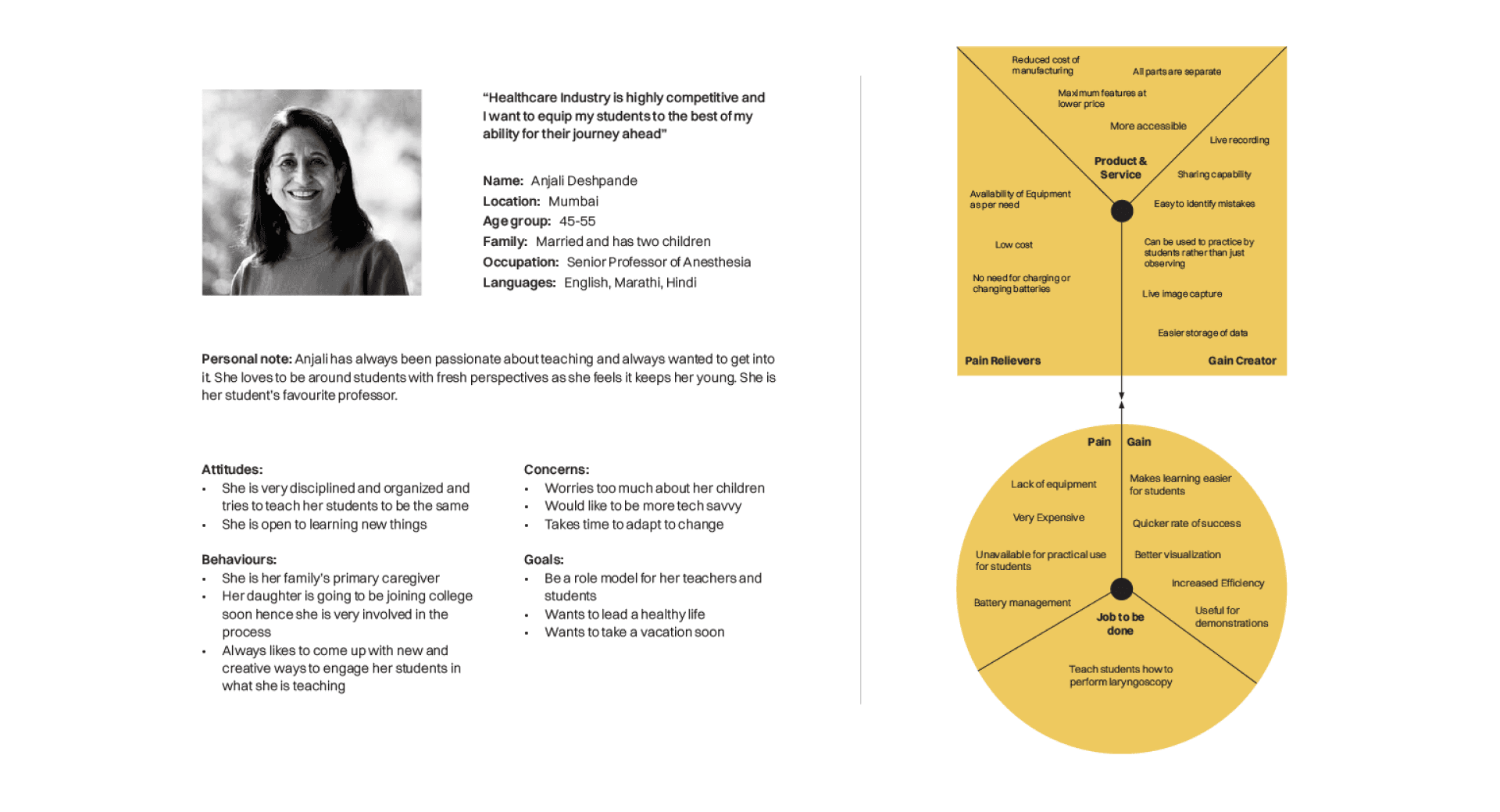
User Persona 2
Key Insights
1
There is a higher need for video laryngoscopes especially during the COVID 19 pandemic as the doctors do not need to get too close to the patient for appropriate visualisation while dealing with COVID positive patients.
3
Most young doctors (25-40 years) would be open to using their smartphone for assistance in laryngoscopy as long as their safety and the patient's safety are not breached, especially while dealing with patients with transmittable diseases.
2
Most teaching hospitals only have one or two poor quality video laryngoscopes available to them despite being a useful tool for teaching and practical demonstration of the procedure for the students as they are incredibly expensive.
4
There is no defined protocol for sterilising electronic parts of the video laryngoscope and only the blades undergo strict sterilisation while other parts like the handle and the video output unit are wiped using an alcohol solution.
Synthesis & Context of Focus
Redefined Brief
Develop a video laryngoscope that can use any smartphone as a video output unit keeping in mind health and safety concerns for the user and the stakeholders involved
Design Criteria
→ Make laryngoscopes more accessible to the lesser privileged hospitals and institutions
→ Develop it to be a useful tool for students in teaching hospitals
→ Make sure to prevent any spread of transmittable diseases between doctors and patients
→ Easily integrate features like recording capability, live image capture with the help of a smartphone which are only seen in higher end video laryngoscopes
→ Relieve any restriction on sterilisation of certain parts due to the presence of electronic components
Target User
Anaesthetists belonging to progressive and community hospitals and professors of anaesthesia in medical colleges and other teaching institutions

Progressives & Community Hospitals

Medical Institutions & teaching Hospitals
Conceptualisation & ideation
Explorations

Concept 1
Concept 2
Concept 3

Concept Validation

Conducting User Validation
I conducted my user validation with a total of five users. it was conducted in two parts - Part A & Part B. Part A was a scoring based section where the scored five parameters: Comfort - Handle Ergonomics, Adjustability - Viewing Angles, Ease of Use - Attachment Mechanics, Functionality - Overall Usage, Aesthetics - Looks for each of the three concepts out of a score of five. Part B was choosing their prefered ideal configuration for the Handle, Phone Attachment, Blade Attachment and the mounting mechanism.

Part A Results
To tally the scores the scores for the concepts, scores for each parameter were totaled and then an average was calculated to get a fair estimation of the perception of each of the parameters across the three concepts. As shown in the figure below we can observe that concept one scored well in its attachment mechanics and also its adjustability in terms of viewing angles however the overall bulky for wasn’t appreciated which affected the overall functionality of the ptoduct. Concept two was best recieved in the aesthetics and the comfort parameters scoring far higher than bothe the other concepts and even the the single hinge for angle adjustment was appreciated by the users for its simplicity. However its threading mechanism for attaching both the top and bottom assemblies were rated the worst across all parameters acroos the study which drastically hampered its overall functionality score. Concept three again was appreciated for its ease of use and simple attachment mechanics however the boxy for of the product wasn’t prefered by many users and also concerns regarding the swivel mechanism for angle adjustment were raised by users.

Part B Results
To tally the results of the ideal configurations picked by individual users each of the options were totaled and a percentage of their occurance was calculated as displayed in the figure below. From this we could clearly observe that concept two had the most prefered handle, slot mechanism was the prefered choice for attaching the phone followed close by the mechanical buttons. However for the blade attachment mechanical buttons were the most prefered by a large margin. When it came to the joinery users prefered the single hinge over the others as they mentioned they only require adjustment in one direction while using the product and having a lot of flexibility in terms of adjustment doesn’t really add value to them.
Conclusion
From the user validation these were the following key points to take away -
Users preferred the form of the second concept the most out of all three presented to them.
Threading mechanisms are the least preferred mechanisms for attachment despite being offered in many video laryngoscopes today.
Slot mechanism and the mechanical buttons were the most popular choices for attachment of the phone assembly and blade attachment respectively.
Users don’t require a lot of adjustability when it comes to viewing angles and providing too much adjustability does not add much value as the users preferred the single hinge over the rest of the joineries.
Therefore we can conclude that the ideal configuration for the final product would have the handle of concept two either slot of mechanical buttons for attachment of the phone assembly and the blade and a singe hinge joinery for adjusting the viewing angle. Based on the following points I began developing the final concept.
Interface Development
From my research it was evident that using smartphones as a video output unit would be beneficial to a lot of smaller hospitals as well teaching institutions. Also referring to “Video laryngoscopy using an Android smartphone: A direct digital technique” from my initial validation section we learnt that the use of CameraFi App from the Google app store was not optimal due to its lack of support therefore developing an interface for using the smartphone in a video laryngoscope was crucial.
Objectives
Easy compatibility with the endoscope camera
Account for human error and any distractions from a smartphone during the procedure
Add features like recording capability and live image capture
Easy to store and share data
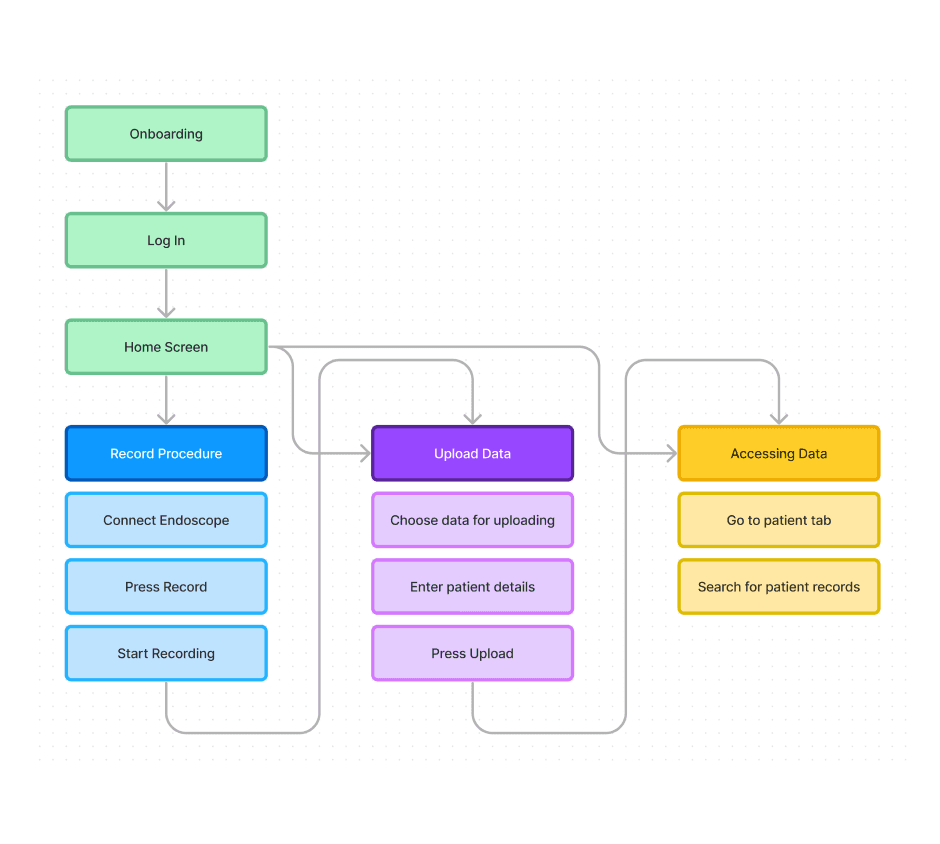
Information Architecture

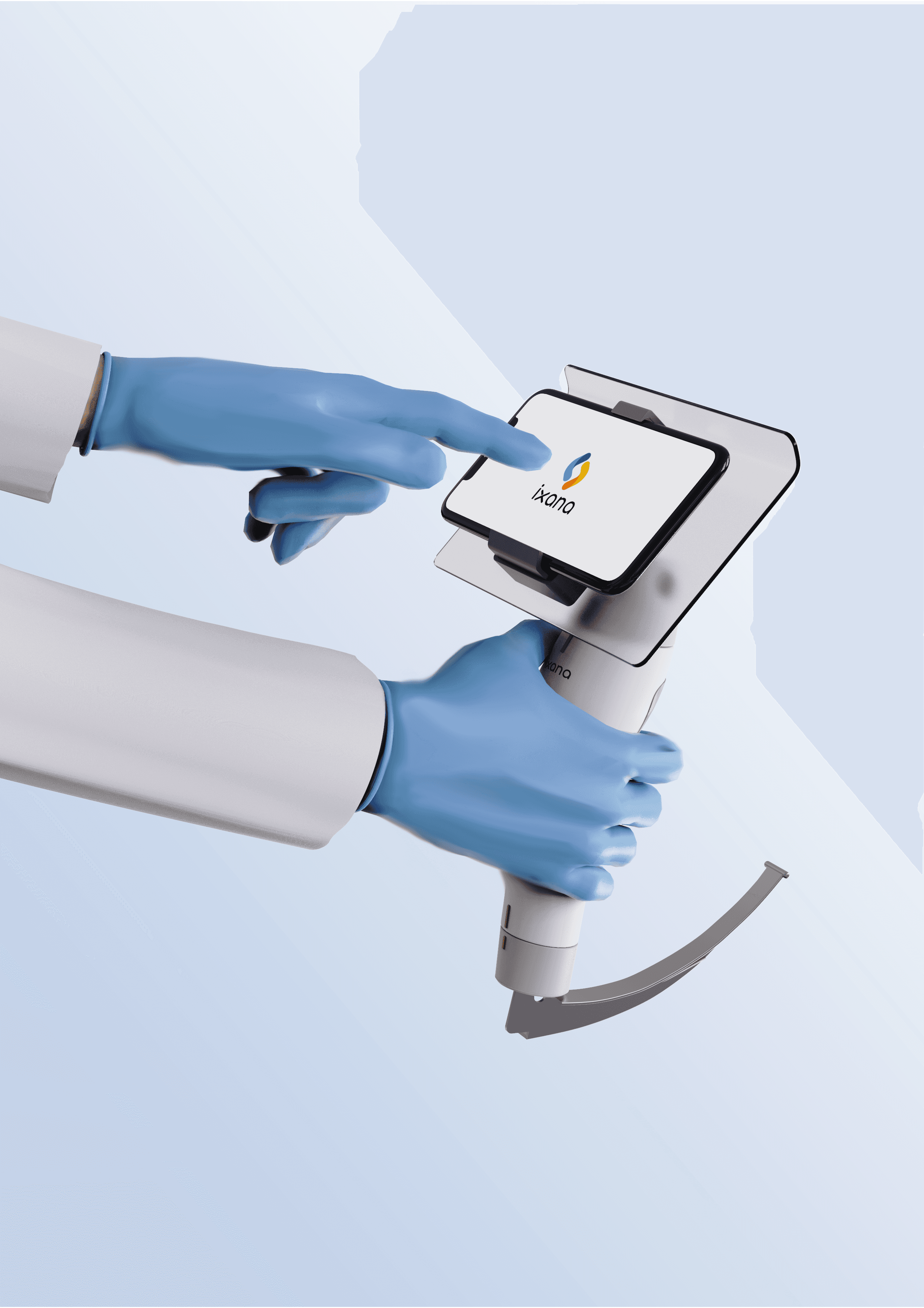
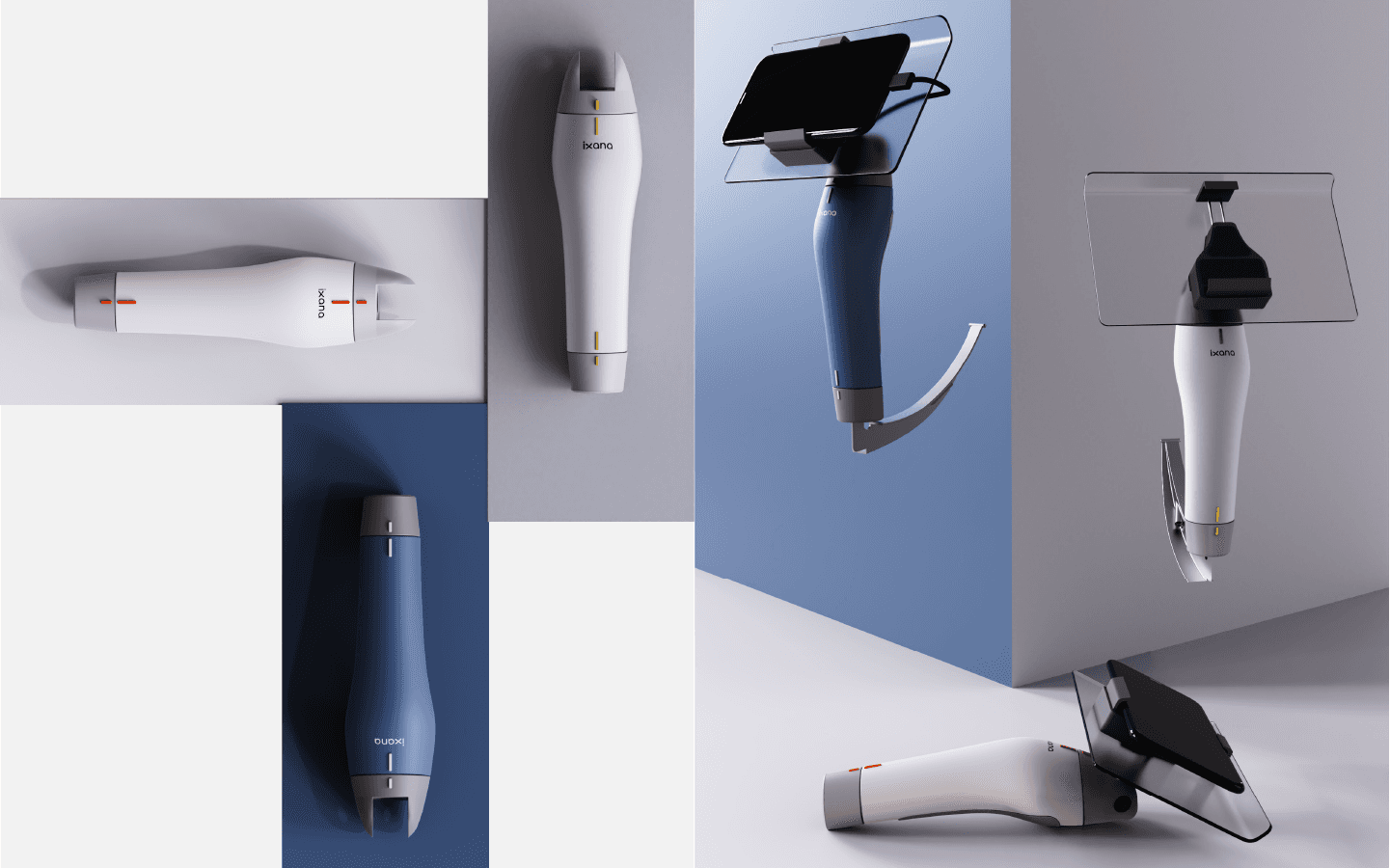
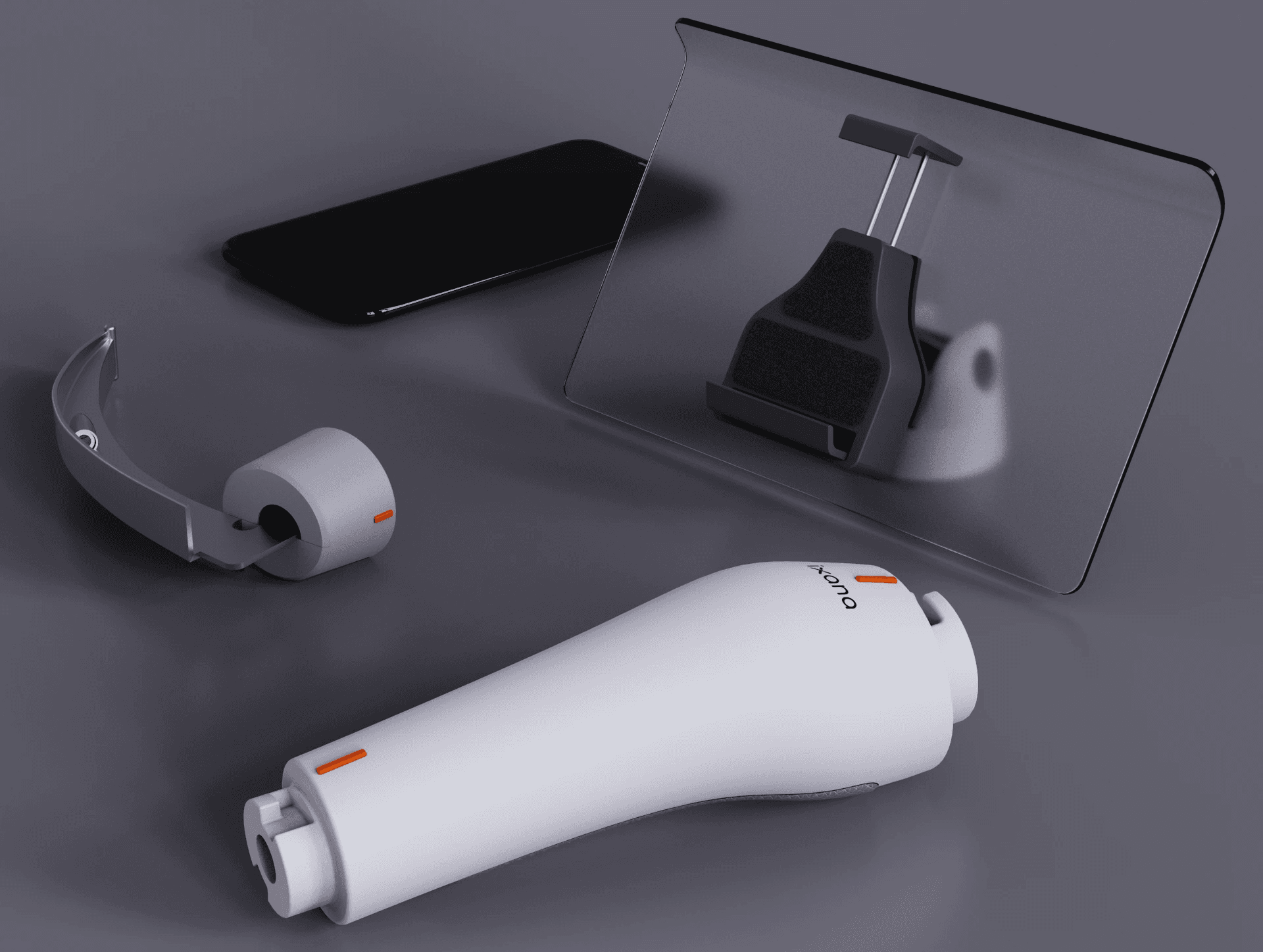
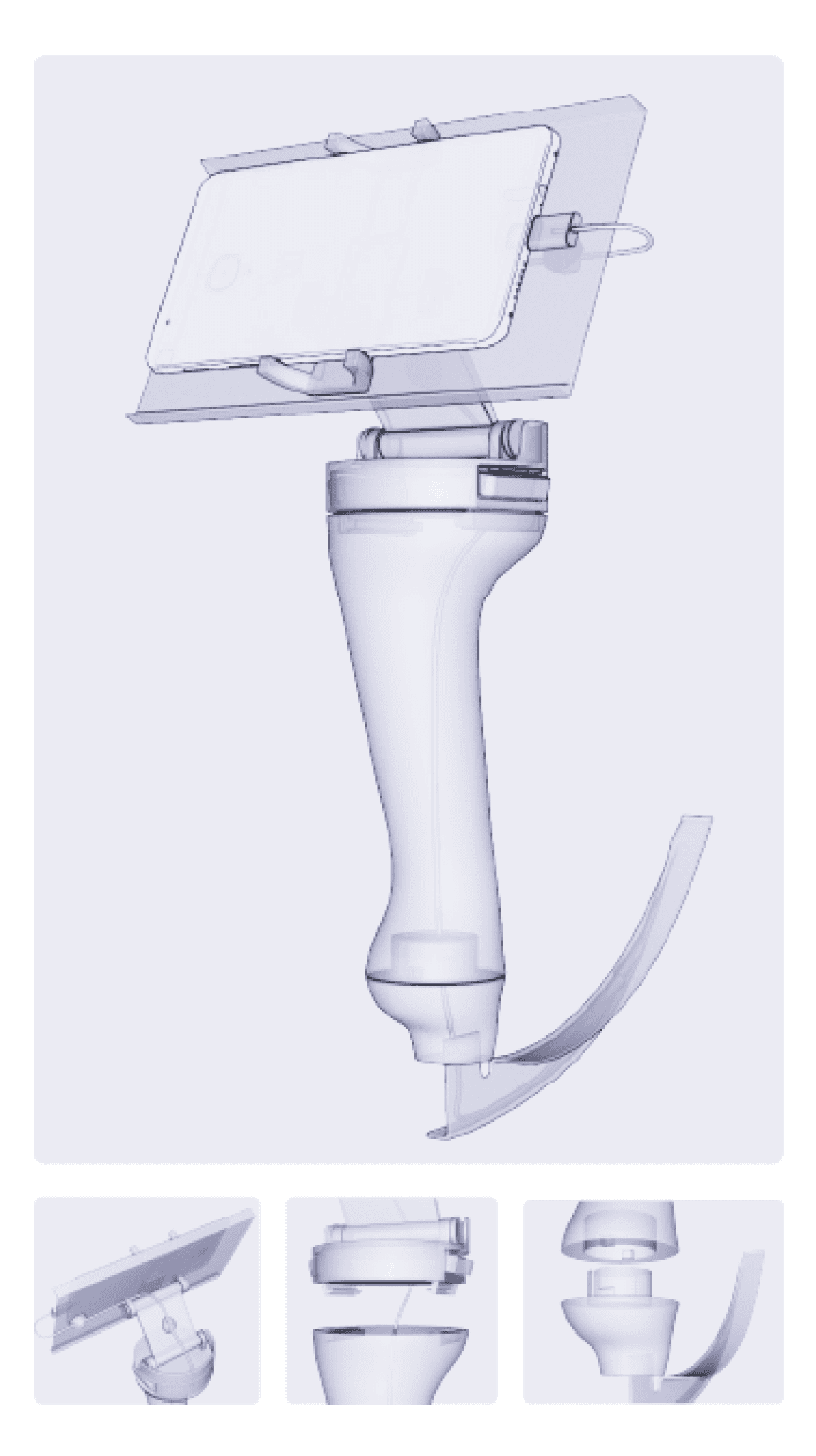
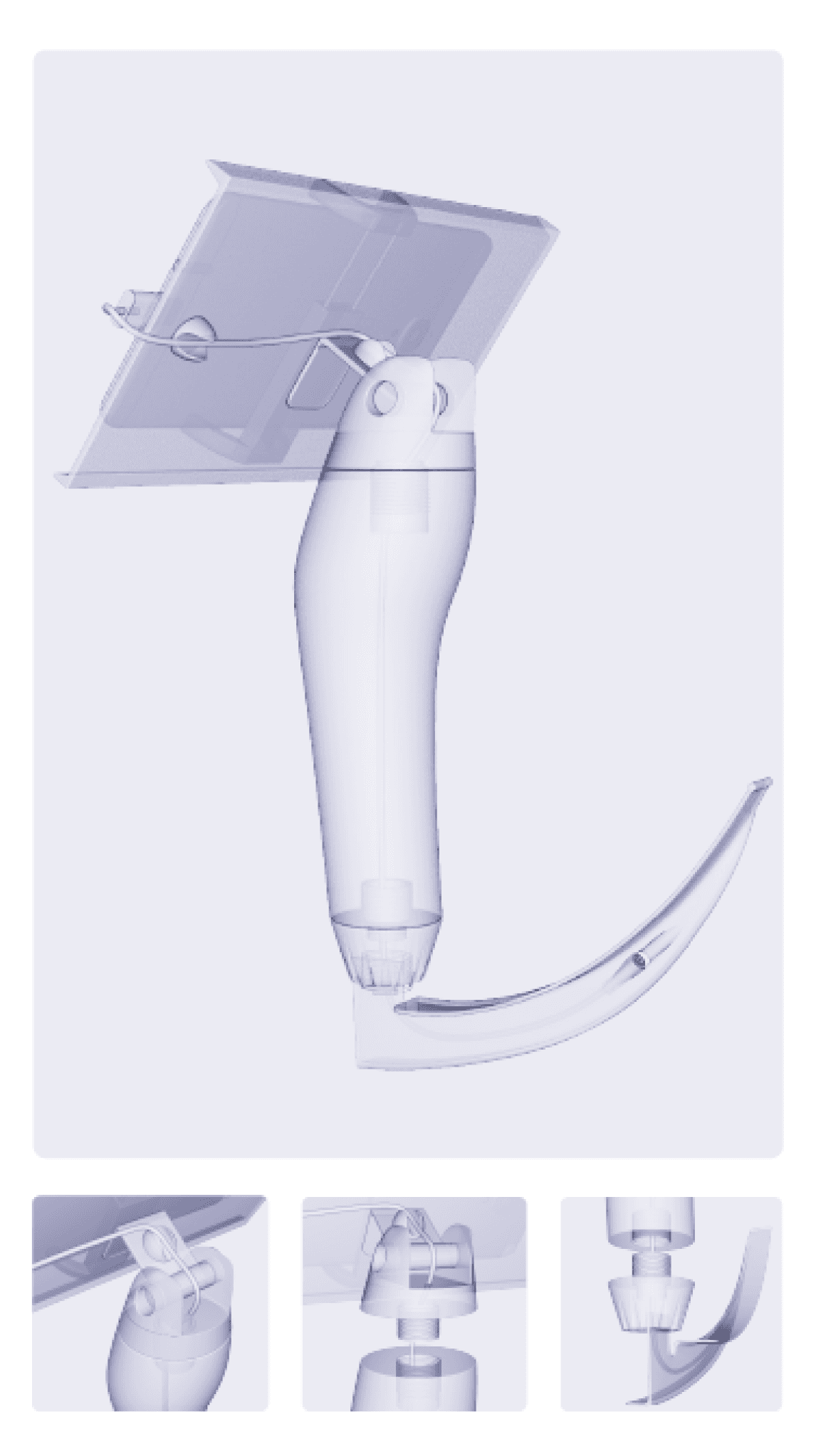
Final Product